Creatinine Clearance
Calculates CrCl according to the Cockcroft-Gault equation.
Calculations must be re-checked and should not be used alone to guide patient care, nor should they substitute for clinical judgment. See our full disclaimer.
Overview
Chronic Kidney Disease (CKD) is defined as abnormalities of kidney structure or function, present for >3 months, with implications for health. Patients with decreased eGFR or albuminuria are at significantly higher risk for Acute Kidney Injury (AKI), progressive kidney failure, and, most notably, cardiovascular disease.
Calculator Selection: eGFR vs. Creatinine Clearance
While often used interchangeably, these metrics have distinct clinical applications based on current regulatory and guideline standards:
eGFR (CKD-EPI 2021): The KDIGO-recommended standard for diagnosing and staging CKD. Current guidelines recommend using the 2021 CKD-EPI creatinine equation without the race variable to ensure equity in clinical practice.
Creatinine Clearance (Cockcroft-Gault): Historically used for drug development. While the FDA and EMA now support using eGFR for drug dosing, Cockcroft-Gault remains the standard for dosing certain narrow-therapeutic index drugs (e.g., DOACs, chemotherapy, lithium), particularly in patients with extremes of body weight or muscle mass.
Recommendation: For drug dosing, review the specific medication label. If the patient is at an extreme of body weight (BMI <18.5 or >30), consider calculating both CrCl and eGFR; if results are discordant, use the more conservative estimate to avoid toxicity.
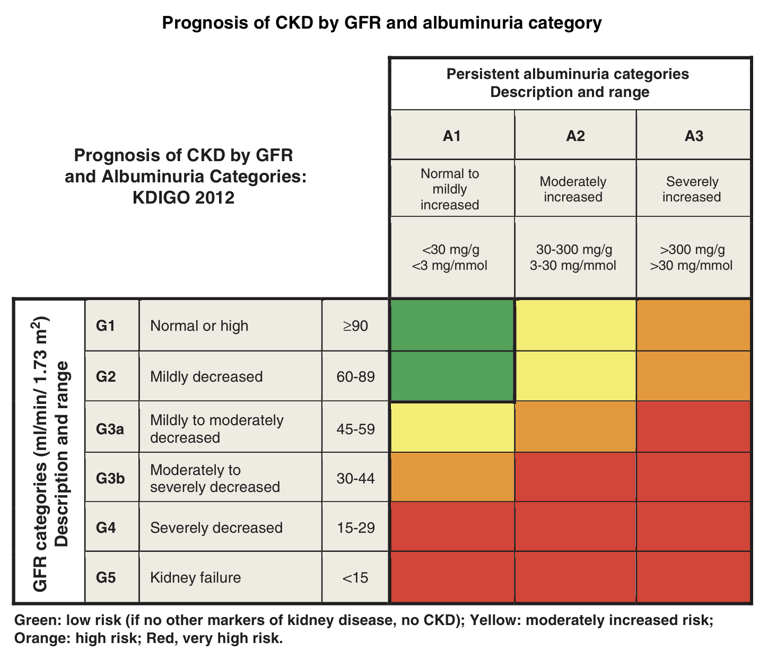
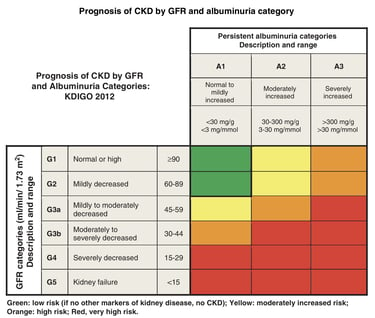
KDIGO Staging (The CGA Framework)
Diagnosis requires classification based on Cause, GFR category, and Albuminuria category (CGA Classification). Do not rely on eGFR alone.
GFR Categories: G1 (>90) to G5 (<15).
Albuminuria Categories: A1 (<30 mg/g), A2 (30–300 mg/g), A3 (>300 mg/g).
Note: A patient with high eGFR but significant albuminuria (e.g., Stage G1A3) is at higher risk than a patient with stable lower eGFR and no albuminuria (e.g., Stage G3aA1).
Management Pillars (KDIGO 2024)
Recent evidence has shifted CKD management from "nephrology-only" to a primary care imperative focusing on four pillars of therapy to delay progression and reduce mortality:
RAAS Inhibition: ACE inhibitors or ARBs (titrated to maximum tolerated dose) for patients with hypertension and albuminuria.
SGLT2 Inhibitors: Recommended for patients with CKD and eGFR ≥20 mL/min/1.73m², regardless of diabetes status, to reduce progression and heart failure.
Blood Pressure Control: KDIGO recommends a target systolic BP <120 mmHg (standardized measurement) if tolerated.
Cardiovascular Risk Reduction: Statin therapy and consideration of GLP-1 RAs for patients with Type 2 Diabetes and CKD.
When to Refer to Nephrology
eGFR <30 mL/min/1.73m² (Stage G4-G5).
Significant albuminuria (ACR >300 mg/g or >30 mg/mmol).
Rapid decline in eGFR (>5 mL/min/1.73m² per year).
Presence of red cell casts or refractory hypertension.
Reference & Further Reading: Guidelines – KDIGO
Feedback
Blog
From Yangon to UK: Decades of Medicine, Moments of Reflection
LINKS:
FIND ME ON:
© 2026. All rights reserved.