VTE - DVT & PE
Venous Thromboembolism
Calculations must be re-checked and should not be used alone to guide patient care, nor should they substitute for clinical judgment. See our full disclaimer.
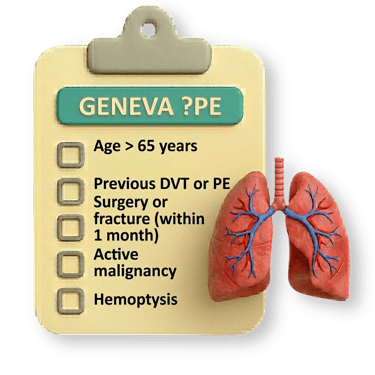
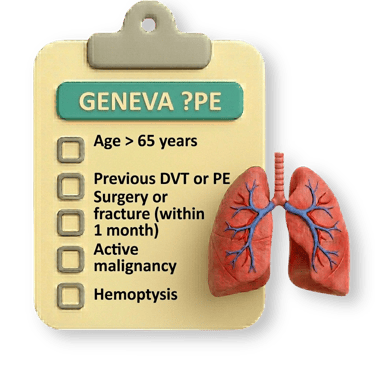
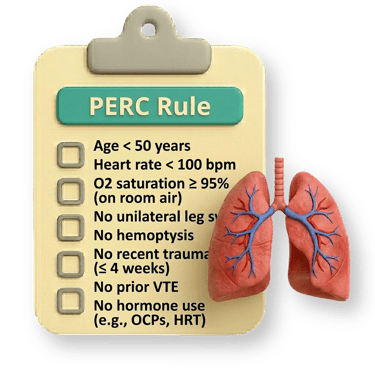
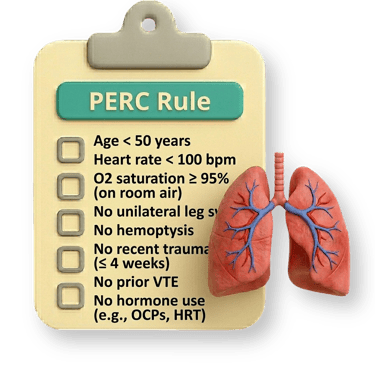
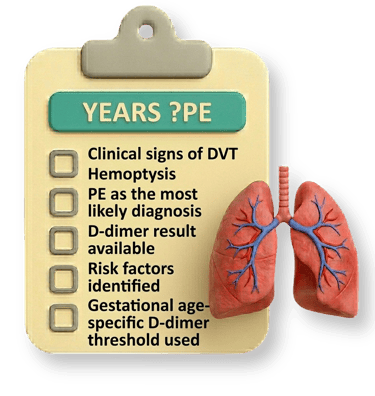
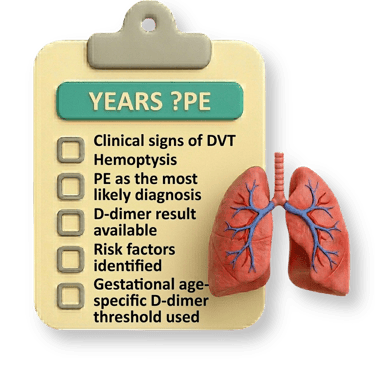
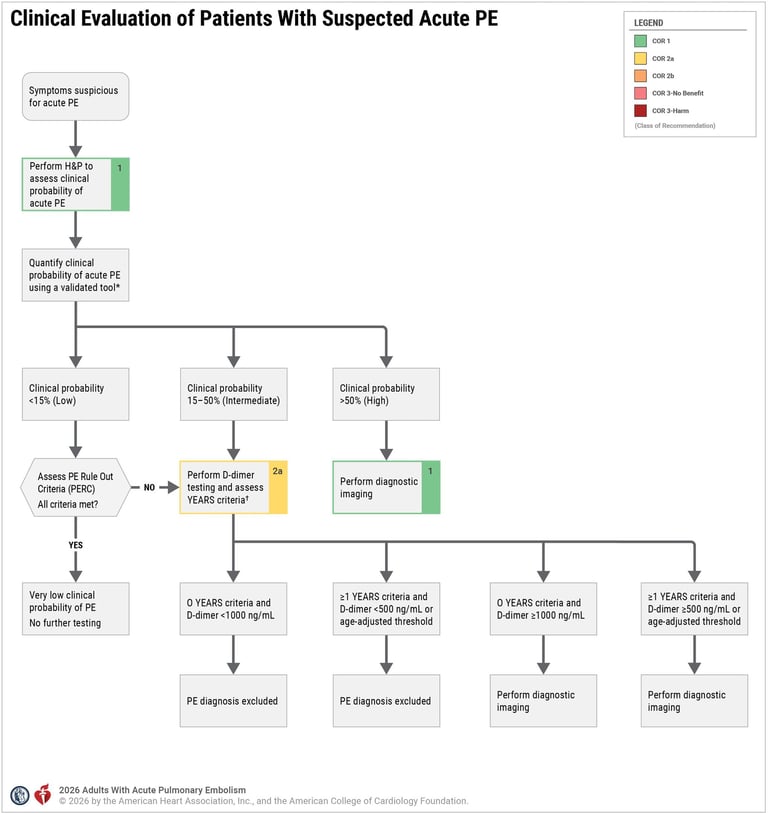
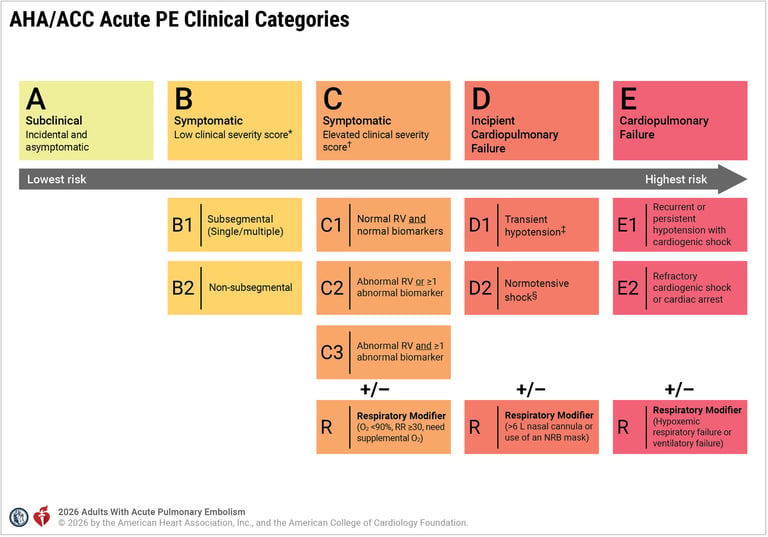
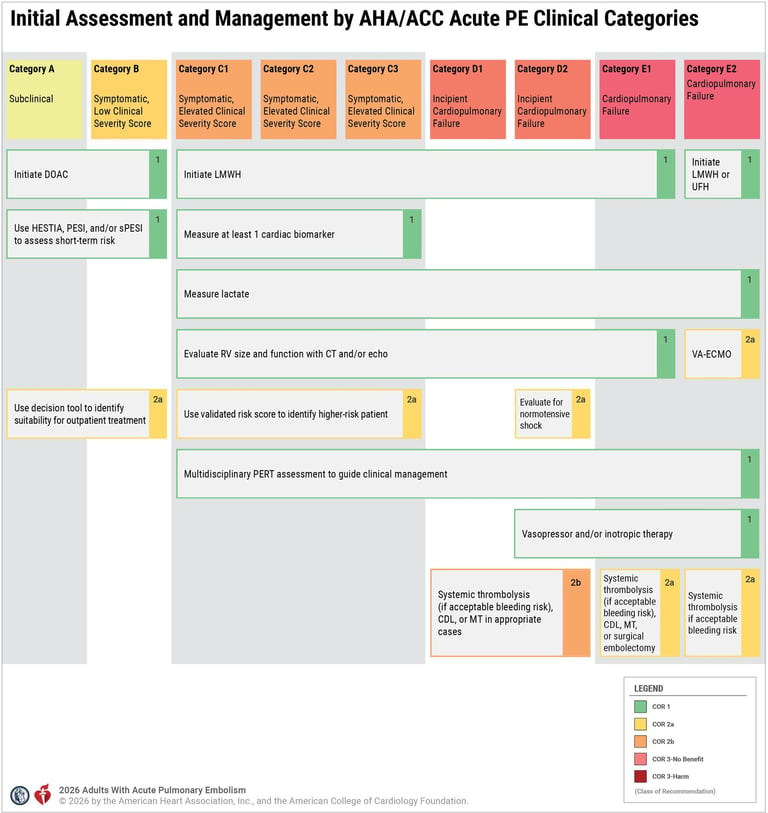
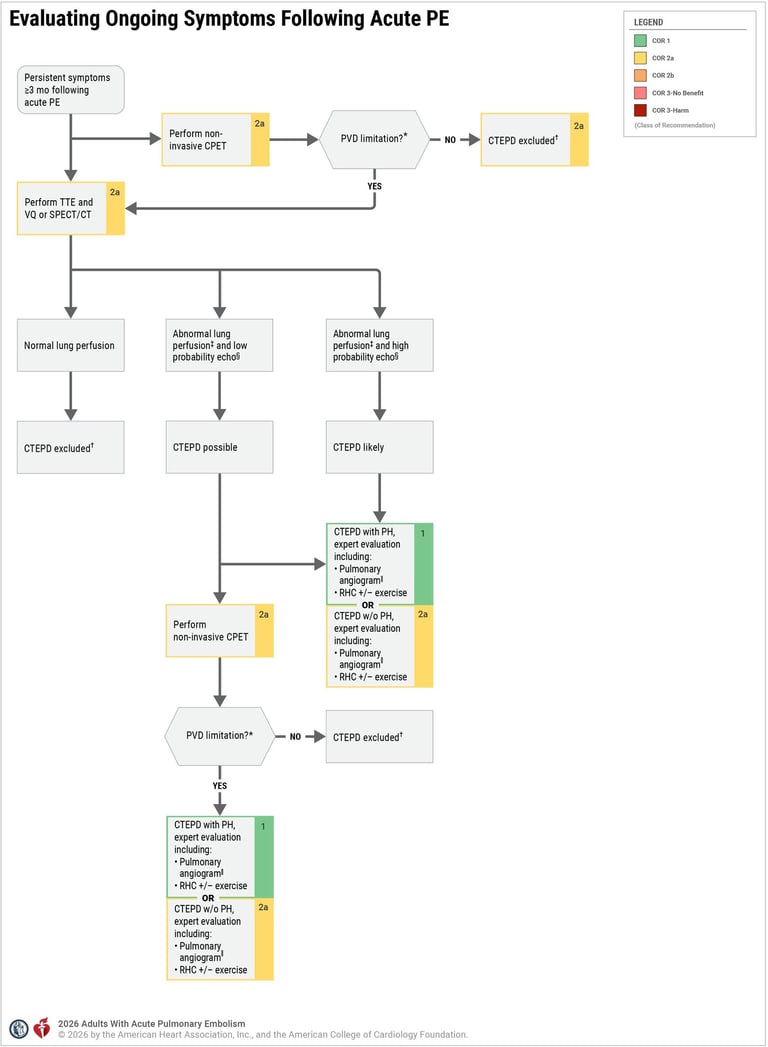
Assessing Probability of DVT/PE
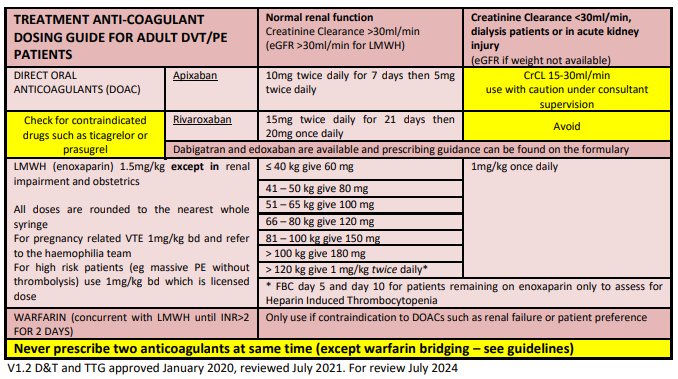
Prescribing LMWH
If, based on VTE risk assessment, a patient is deemed to have a need for pharmacological VTE prophylaxis, the first-line choice of prophylaxis will be a low molecular weight heparin (LMWH).
Body weight, renal function (calculated as creatinine clearance [CrCl] using Cockcroft-Gault equation – eGFR should not be used as it is not equivalent) and individual contraindications/bleeding risk factors should be checked before prescribing.
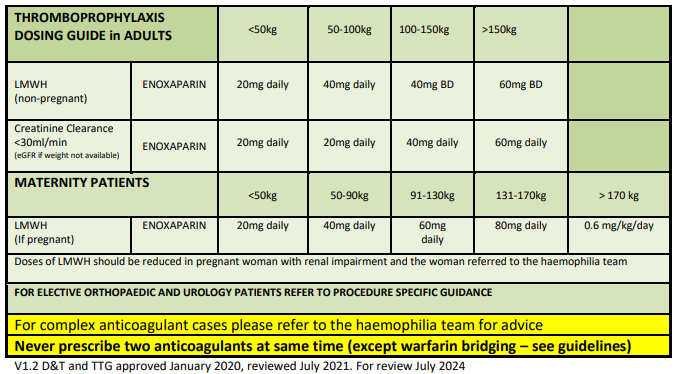
(Prophylaxis)
(Treatment)
* Source: Derbyshire Joint Area Prescribing Committee (JAPC)
Download Links
** Source: Gloucestershire Hospital
Blog
From Yangon to UK: Decades of Medicine, Moments of Reflection
LINKS:
FIND ME ON:
© 2026. All rights reserved.