Takotsubo in an Ageing World
Inspire global health readers with a real Takotsubo “broken heart syndrome” case from GLOBEHEAL 2026, exploring MINOCA, geriatric cardiology, psychosocial stress, and the power of cardiac MRI in modern diagnosis.
PROFESSIONAL
Dr Zaw
2/18/20267 min read
The first time I saw the angiogram, my brain refused to believe it. The numbers and the ECG were screaming “heart attack,” yet the coronary arteries on the screen were almost pristine. In that moment, presenting my case at the 9th Global Public Health Conference (GLOBEHEAL 2026) felt like more than a conference opportunity to improve my IMT application scoring points — it became a chance to tell the story of a heart that broke without a blockage, and what that means for global health.
My first experience as the first author and presenter at a global health conference
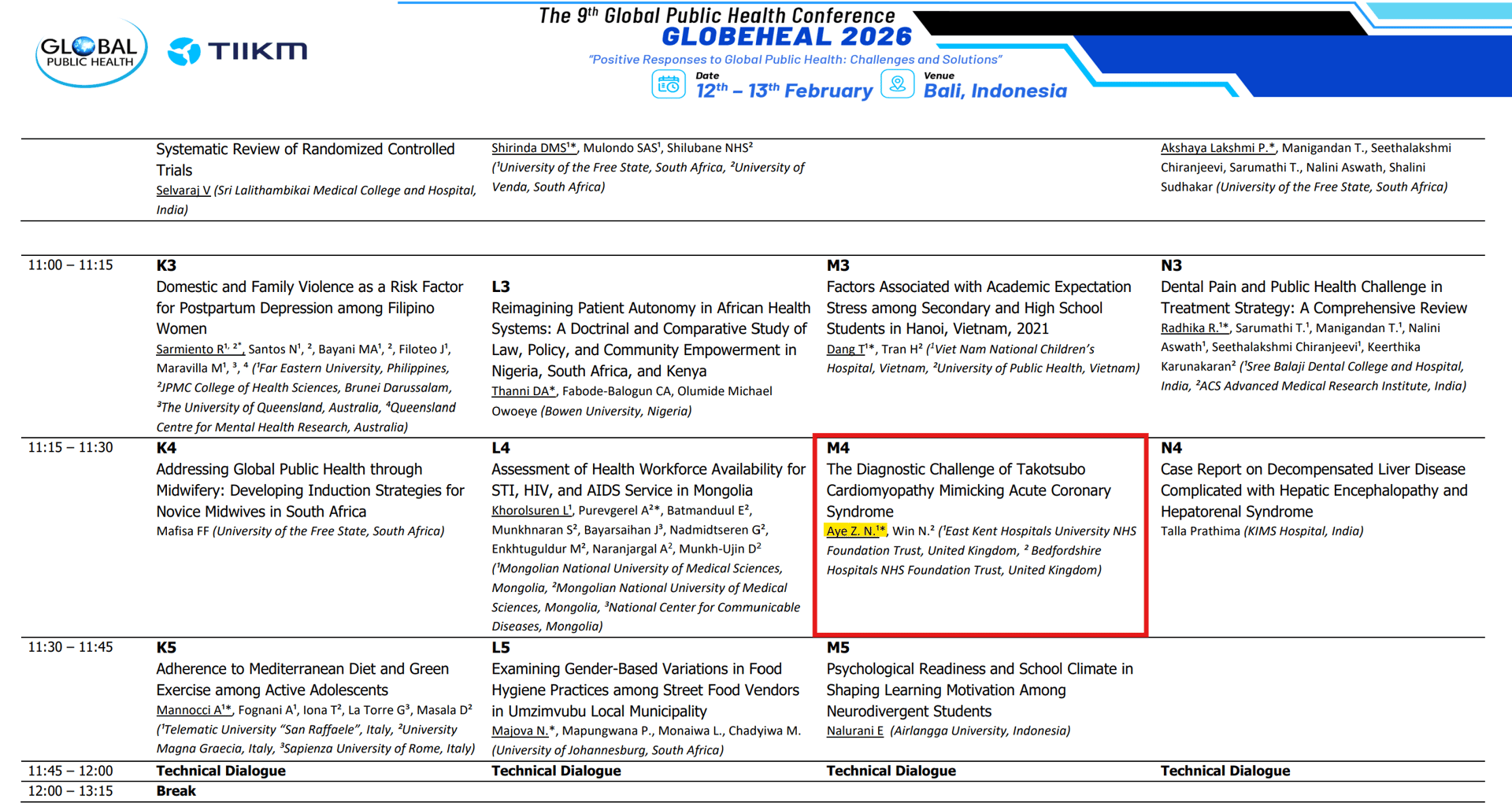
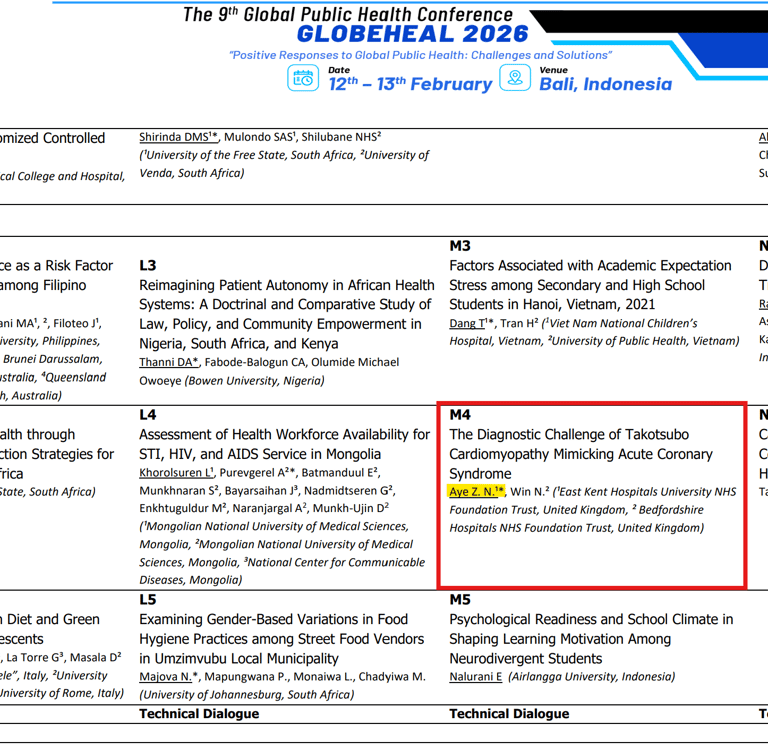
While GLOBEHEAL 2026 was soaking up the sun in Bali, I was soaking up the fluorescent lights of the hospital in the dull and chilly UK winter. Like many clinicians whose professional ambitions are currently outperforming their travel budgets, I joined virtually as an oral presenter. I was on the programme under the theme of mental Health and psycho-social wellbeing, speaking about a single 81‑year‑old woman whose chest pain journey encapsulated some of the biggest questions we face in modern medicine: ageing, complex comorbidities, psychosocial stress, and the limits of our diagnostic assumptions.
Presenting virtually to a room full of global experts—from NGO workers to policy-makers—felt like a high-stakes tightrope walk. As a first-time oral presenter, the 'imposter syndrome' was real, but the experience was ultimately empowering. It’s not every day you get to bridge the gap between a freezing UK winter and a global stage with just a laptop and a stable Wi-Fi connection.
The woman whose heart broke twice
The story started, as so many do, with chest pain.
She was 81, with a long medical history behind her: multiple sclerosis, treated breast cancer in remission following surgery, chemotherapy, and radiotherapy, hypertension, gastro‑oesophageal reflux, hiatus hernia, and a past smoking habit. She was not the stereotypical frail, bed‑bound patient; she swam, danced, lived independently, and carried a Rockwood frailty score of 4. In many ways, she represented the “new older adult”—medically complex but determinedly active.
Her first contact with healthcare for this episode was almost mundane. She presented with chest discomfort to her GP and was treated as a chest infection, receiving oral antibiotics. When things didn’t settle, she ended up in hospital, where the working diagnosis became community‑acquired pneumonia and Intravenous antibiotics were started. The story, at this point, looked like a fairly standard respiratory pathway for an older patient.
Then the heart started to speak more clearly.
Her chest pain persisted, now with discomfort radiating to the left shoulder. The ECG changed: a new left bundle branch block (LBBB) and T‑wave inversions. Troponin came back significantly elevated—over 2800 ng/L. The combined picture of ongoing pain, LBBB, and high troponin triggered what most of us are trained to do: treat as Acute Coronary Syndrome (ACS).
In those crucial early hours, the world is black‑and‑white: time is myocardium, and delays cost muscle. She was managed appropriately as suspected ACS and sent promptly for urgent coronary angiography.
That’s where the narrative bent.
When the arteries don’t match the story
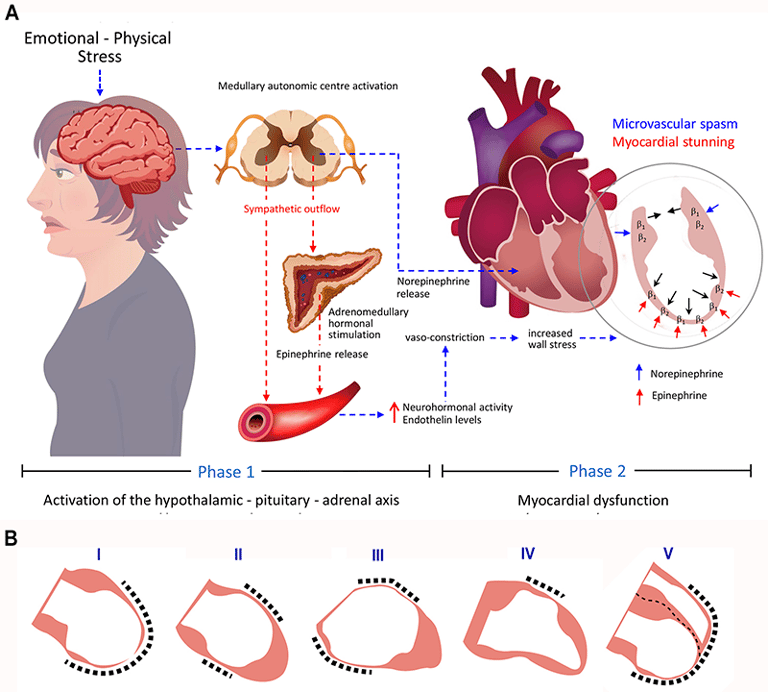
On angiography, her coronary arteries were essentially non‑obstructive. There was some minor impairment in the apical left anterior descending artery, but nothing that explained the severity of her presentation. Instead, the left ventriculogram showed classic apical ballooning—a hallmark of Takotsubo cardiomyopathy.
What looked and behaved like a heart attack was, in fact, something else.
We now had a different acronym to consider: MINOCA—Myocardial Infarction with Non‑Obstructive Coronary Arteries. This is the grey zone where patients have a “heart attack‑like” picture but no significant blockage. Within that category lies Takotsubo cardiomyopathy, often described as “broken heart syndrome,” frequently triggered by intense emotional or physical stress. When I revisited her social history during ward round, she mentioned that she had been under a lot of stress when her daughter was unwell and moving to nursing home a few months ago. This case reminded me how often we anchor on the first plausible diagnosis and how critical it is to keep revisiting the question: “What else could this be?”
Role of CMR
To move from strong suspicion to firm diagnosis, we turned to cardiac MRI. CMR has become increasingly indispensable in MINOCA workups, allowing us to differentiate between myocarditis, infarction, Takotsubo, and other pathologies that can present with similar biochemical and ECG profiles.
Her CMR showed mild apical hypokinesia and evidence of partially recovered left ventricular function—consistent with the transient nature of Takotsubo. There was myocardial inflammation in the apical segments and, interestingly, in the pericardium, pointing to associated pericarditis. Crucially, there was no evidence of myocardial infarction.
Now, the pieces fit.
What started as a presumed ACS was, in the end, Takotsubo cardiomyopathy with co‑existing pericarditis—a rarer combination that added another layer of complexity to an already challenging case. The diagnosis shifted her long‑term management and prognosis, but it also changed something in us, the clinicians, about how we think.
This was the story I brought to GLOBEHEAL 2026.
From one patient to a global pattern
In my talk, I placed this single case in the broader context of global health. On the face of it, Takotsubo in an older woman in a UK hospital might look like a niche cardiology topic rather than a “global health” issue. But the more I reflected, the more it felt emblematic of three wider trends.
First, populations are ageing across the world. Geriatric cardiology is no longer a concern of high‑income countries alone. Older adults with multiple comorbidities and complex psychosocial lives are being treated in hospitals from Bali to Birmingham to Bangkok. The challenge of distinguishing ACS from its mimics in this group—where both under‑ and over‑treatment carry risk—is universal.
Second, non‑communicable diseases (NCDs) and mental health are increasingly intertwined. Takotsubo cardiomyopathy is often triggered by intense emotional stress—bereavement, shock, anxiety. Here was a heart literally shaped by stress. When we talk about NCDs in the global health arena, we often think in terms of numbers—hypertension rates, diabetes prevalence, stroke burden. Cases like this remind us that behind those statistics are lives lived under strain, and that the body keeps the score.
Third, diagnostic equity matters. Access to coronary angiography and CMR is far from uniform worldwide. In some settings, this patient might have been labelled indefinitely as “post‑MI,” with all the implications that carries for medication, insurance, and identity. Global health is not only about providing basic access; it is also about providing the right diagnosis and avoiding unnecessary long‑term therapies when the pathology is actually different.
Standing (virtually) in front of an international audience, I realised that my patient’s story resonated with cardiologists, internists, GPs, and public health professionals in different ways. For some, the imaging was the main point of interest. For others, it was the psychosocial trigger. For many, it was the reminder that older patients are not just “frail” but complex, resilient, and sometimes unexpectedly vulnerable.
Presenting at GLOBEHEAL 2026 as a virtual oral presenter was its own kind of stress test. There is something uniquely challenging about speaking into a camera, trying to gauge reactions from a grid of muted microphones and tiny faces—or sometimes just initials. You can’t feel the room in the same way, yet you know the reach may be even larger.
I had structured my slides deliberately simply: minimal text, clear images, and a narrative arc that took the audience from “typical” chest pain through each turning point—first misdirection, then ACS management, then angiography surprise, and finally CMR confirmation. The virtual format with time limit forced me to be disciplined with my wording and pacing. When you can’t rely on theatrical body language or eye contact, clarity becomes your most powerful tool.
As I worked on this case, questions came in about:
How we balance the urgency of ACS protocols with awareness of conditions like Takotsubo.
Whether we should be doing CMR more routinely in MINOCA cases.
How we can better integrate psychosocial assessment into cardiology workups, especially in older adults.
Lessons I took home
When the session ended and I closed my laptop, the experience didn’t feel finished. If anything, presenting at GLOBEHEAL sharpened the lessons I had already been slowly learning from this patient.
A few of the key ones:
Keep Takotsubo on the differential in MINOCA.
A high troponin and dramatic ECG do not always equal obstructive coronary disease. Particularly in older women with recent stressors, Takotsubo deserves serious consideration.Don’t stop at the angiogram.
Non‑obstructive coronaries are not the end of the story; they are the doorway to a different set of questions. CMR, when available, can provide the missing chapter in the diagnostic narrative, differentiating infarction, myocarditis, and Takotsubo.Look for the story behind the numbers.
Biomarkers and imaging are essential, but so is asking, “What has this person just been through?” Emotional stress, life events, and mental health can profoundly shape cardiac presentations.Older adults deserve nuanced thinking.
It is easy to fall into stereotypes—either under‑investigating because “they’re old” or over‑medicalising without considering quality of life and psychosocial factors. This patient reminded me that age does not simplify medicine; it makes it richer and more complex.Global health is also about better everyday medicine.
Conferences like GLOBEHEAL often showcase big themes: pandemics, climate change, health policy. But they also create space for quieter stories—like an older woman with Takotsubo—that embody how improving diagnosis, communication, and person‑centred care is itself a form of global health work.
From one case to a wider voice
Receiving my certificate as a virtual oral presenter was a satisfying moment—a formal recognition of the hours spent reviewing notes, refining slides, and rehearsing a 12‑minute talk. But the more lasting reward has been the reflection that followed.
This case changed how I think about chest pain, about ageing, and about the emotional lives of my patients. It reminded me that global health is not something that happens “out there” in distant policies and projects; it is also what happens in a single cubicle, a single cath lab, a single conversation with one older woman and her family.
Writing this blog is, in a way, a continuation of that conversation—just with a wider audience. If there is one message, I hope readers take away, it is this: "listen to the heart, but also to the story around it". Sometimes, the most important diagnoses are made not just with a troponin result or an angiogram, but with curiosity, humility, and a willingness to keep asking, “Could this be something else?”
In an increasingly connected world, our patients’ stories do not stop at the hospital door, and neither should our learning. Conferences like GLOBEHEAL provide the bridge between bedside and global dialogue. I feel fortunate that one woman’s “broken heart” could become a chance to build that bridge a little further.
Blog
From Yangon to UK: Decades of Medicine, Moments of Reflection
LINKS:
FIND ME ON:
© 2026. All rights reserved.